Acoustic Reflex Testing
Evoked Potentials Guides
Overview
Short-latency potentials evoked through activation of vestibular receptors using sound or vibration are referred to as vestibular evoked myogenic potentials (VEMP). VEMP are generated by modulated electromyographic signals and recorded with surface electrodes. A VEMP recorded from the sternocleidomastoid muscle is commonly referred to as the cervical vestibular-evoked myogenic potentials (cVEMP). A VEMP recorded from the inferior oblique muscle has been termed the ocular vestibular-evoked myogenic potentials (oVEMP). These reflexes appear to originate from the otolith organs and thus complement existing methods of vestibular assessment, which are mainly based upon canal function. VEMP testing is used clinically to assess the function of the vestibular system, including the saccule, utricle, and the inferior and superior portions of the vestibular nerve.
Types of VEMP
cVEMP
The cVEMP is part of the evaluation of a patient experiencing vestibular disorders such as dizziness or vertigo. The cVEMP is generated from the saccule (otolith organ in the cochlea) in response to a loud sound and is recorded from the contracted sternocleidomastoid (SCM) muscle. The cVEMP is not affected by sensorineural hearing loss but may be reduced or absent in the presence of conductive hearing loss. Therefore, audiologic evaluation is necessary prior to performing VEMP testing.
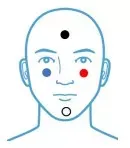
Below is a commonly used the cVEMP montage.
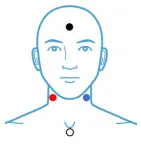
Red (right) and blue (left) electrodes should be placed on the largest part of the SCM muscle which is approximately halfway between the ear and the sternum when the head is turned as shown below:
Note: This montage will result in downward deflection for P1 and upward deflection for N1.
Common Test Settings
- Stimulus: 500 Hz Tone Burst
- Duration: 4 cycles
- Envelop: Blackman
- Phase: Alternating
- Intensity: 90-95 dBnHL
- Transducer: Insert Earphones
- Rate: 5.1 clicks/sec
- Sweeps: 100, replicated
- Gain: 5k*
- High Pass Filter: 10 Hz
- Low Pass Filter: 1000 Hz
- Window: 50-100 msec
The amplitude of the cVEMP is directly affected by the amount of the neck muscle contraction; therefore, efforts should be made to ensure this contraction is equal for both right and left ear recordings. If EMG feedback to the patient is not available, utilizing the procedure shown below can assist in keeping the contraction approximately equal when both ears are evaluated.
To record a cVEMP, place the patient in a reclining position (similar to caloric positioning during VNG). Instruct the patient to turn their head away from the ear being stimulated and to lift their head off the table slightly (as shown below) when they hear the stimulus. The patient should be informed that the stimulus will be loud but only present a short time.
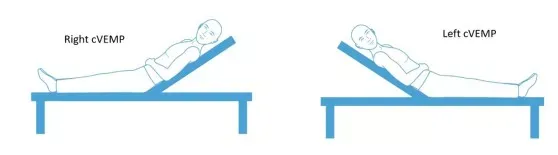
Instruct the patient to lift their head and immediately start the recording. Replicate the response and repeat in the other ear. Keep in mind that the patient may fatigue quickly. Depending on the purpose of the cVEMP test, a cVEMP threshold may be obtained by decreasing intensity until cVEMP is no longer visible.
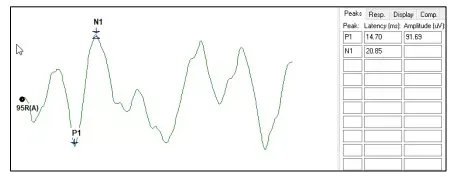
The cVEMP can be marked as follows. Drag the bottom marker of P1 to N1 obtain the amplitude.
- P1 occurs about 14 - 20.5 msec
- N1 occurs about 22 - 29.3 msec
Latency assists in marking the waveform but is not routinely used in analysis.
The cVEMP is analyzed by calculating the amplitude asymmetry (%) between ears. The formula is:

An asymmetry ratio above approximately 30 - 40% is considered an abnormal finding.
oVEMP
The oVEMP test is often used in the evaluation of a patient experiencing dizziness or vertigo. The oVEMP potential is a response generated from the utricle and superior vestibular nerve in response to air conducted stimuli. The oVEMP potential primarily measures utricular function. oVEMP responses are recorded from extra-ocular muscles slightly below the eye contralateral to stimulation. Normal oVEMP responses are obtained at approximately 95 dBnHL using a 500 Hz tone burst.
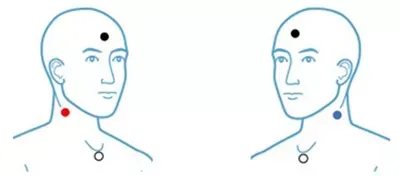
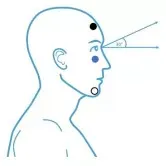
Below is a commonly used oVEMP montage. oVEMPs are recorded contralateral to ear being stimulated therefore the left (blue) lead should be placed under the right eye and the right (red) lead placed under the left eye.
Note: The above montage results in a downward deflection for N1 and an upward deflection for P1.
Common Test Settings
- Stimulus: 500 Hz Tone Burst
- Duration: 4 cycles
- Envelop: Blackman
- Phase: Alternating
- Intensity: 95 dBnHL
- Transducer: Insert Earphones
- Rate: 5.1 clicks/sec
- Sweeps: 100, replicated
- Gain: 100k
- High Pass Filter: 1 Hz
- Low Pass Filter: 1000 Hz
- Window: 50 - 80 msec
The patient should be sitting upright and instructed to gaze upward about 30 degrees. It may be helpful to place a mark in the exam room and ask the patient to gaze at the mark for the duration of the test.
Begin the collection ensuring the patient the patient is gazing upward for the duration of the recording. Replicate and repeat the test in the opposite ear.
The oVEMP consists of an N1 and P1 with approximate latencies as shown. Obtain an amplitude measure by dragging the bottom marker of N1 up to the P1 peak.
- N1 Latency 10 - 12 ms
- P1 Latency 15 - 17 ms
The oVEMP is analyzed by calculating the amplitude asymmetry (%) between ears. The formula is:

An amplitude asymmetry greater than approximately 35 - 40% is considered abnormal.